Each capsule contains 100 mg or 200 mg celecoxib.
Excipients/Inactive Ingredients: Capsules content: lactose monohydrate, sodium laurilsulfate, povidone, croscarmellose sodium, magnesium stearate.
100 mg capsule shell: White body: gelatin, titanium dioxide (C.I. 77891).
Light-blue head capsule: gelatin, titanium dioxide (C.I. 77891), indigo carmine (FDC&C Blue 2).
200 mg capsule shell: White capsule: gelatin, titanium dioxide (C.I. 77891).
Pharmacotherapeutic group: Non-steroidal anti-inflammatory and antirheumatic drugs, NSAIDs, Coxibs. ATC code: M01AH01.
Pharmacology: Pharmacodynamics: Mechanism of action: Celecoxib is an oral, selective, COX-2 inhibitor within the clinical dose range (200-400 mg daily). No statistically significant inhibition of COX-1 (assessed as ex vivo inhibition of thromboxane B2 [TxB2] formation) was observed in this dose range in healthy volunteers.
Pharmacodynamic effects: Cyclooxygenase is responsible for generation of prostaglandins. Two isoforms, COX-1 and COX-2, have been identified. COX-2 is the isoform of the enzyme that has been shown to be induced by pro-inflammatory stimuli and has been postulated to be primarily responsible for the synthesis of prostanoid mediators of pain, inflammation, and fever. COX-2 is also involved in ovulation, implantation and closure of the ductus arteriosus, regulation of renal function, and central nervous system functions (fever induction, pain perception and cognitive function). It may also play a role in ulcer healing. COX-2 has been identified in tissue around gastric ulcers in humans but its relevance to ulcer healing has not been established.
The difference in antiplatelet activity between some COX-1 inhibiting NSAIDs and COX-2 selective inhibitors may be of clinical significance in patients at risk of thrombo-embolic reactions. COX-2 selective inhibitors reduce the formation of systemic (and therefore possibly endothelial) prostacyclin without affecting platelet thromboxane.
Celecoxib is a diaryl-substituted pyrazole, chemically similar to other non-arylamine sulfonamides (e.g. thiazides, furosemide) but differs from arylamine sulfonamides (e.g. sulfamethoxizole and other sulfonamide antibiotics).
A dose-dependent effect on TxB2 formation has been observed after high doses of celecoxib. However, in healthy subjects, in small multiple dose studies with 600 mg BID (three times the highest recommended dose) celecoxib had no effect on platelet aggregation and bleeding time compared to placebo.
Clinical efficacy and safety: Several clinical studies have been performed confirming efficacy and safety in osteoarthritis, rheumatoid arthritis and ankylosing spondylitis. Celecoxib was evaluated for the treatment of the inflammation and pain of osteoarthritis of the knee and hip in approximately 4200 patients in placebo and active controlled trials of up to 12 weeks duration. It was also evaluated for treatment of the inflammation and pain of rheumatoid arthritis in approximately 2100 patients in placebo and active controlled trials of up to 24 weeks duration. Celecoxib at daily doses of 200 mg - 400 mg provided pain relief within 24 hours of dosing. Celecoxib was evaluated for the symptomatic treatment of ankylosing spondylitis in 896 patients in placebo and active controlled trials of up to 12 weeks duration. Celecoxib at doses of 100 mg BID, 200 mg QD, 200 mg BID and 400 mg QD in these studies demonstrated significant improvement in pain, global disease activity and function in ankylosing spondylitis.
Five randomised double-blind controlled studies have been conducted including scheduled upper gastrointestinal endoscopy in approximately 4500 patients free from initial ulceration (celecoxib doses from 50 mg - 400 mg BID). In twelve week endoscopy studies celecoxib (100 - 800 mg per day) was associated with a significantly lower risk of gastroduodenal ulcers compared with naproxen (1000 mg per day) and ibuprofen (2400 mg per day). The data were inconsistent in comparison with diclofenac (150 mg per day). In two of the 12-week studies the percentage of patients with endoscopic gastroduodenal ulceration was not significantly different between placebo and celecoxib 200 mg BID and 400 mg BID.
In a prospective long-term safety outcome study (6 to 15 month duration, CLASS study), 5,800 osteoarthritis and 2,200 rheumatoid arthritis patients received celecoxib 400 mg BID (4-fold and 2-fold the recommended osteoarthritis and rheumatoid arthritis doses, respectively), ibuprofen 800 mg TID or diclofenac 75 mg BID (both at therapeutic doses). Twenty-two percent of enrolled patients took concomitant low-dose acetylsalicylic acid (≤325 mg/day), primarily for cardiovascular (CV) prophylaxis. For the primary endpoint complicated ulcers (defined as gastrointestinal bleeding, perforation or obstruction) celecoxib was not significantly different than either ibuprofen or diclofenac individually. Also for the combined NSAID group there was no statistically significant difference for complicated ulcers (relative risk 0.77, 95 % CI 0.41-1.46, based on entire study duration). For the combined endpoint, complicated and symptomatic ulcers, the incidence was significantly lower in the celecoxib group compared to the NSAID group, relative risk 0.66, 95 % CI 0.45-0.97 but not between celecoxib and diclofenac. Those patients on celecoxib and concomitant low-dose acetylsalicylic acid experienced 4-fold higher rates of complicated ulcers as compared to those on celecoxib alone. The incidence of clinically significant decreases in haemoglobin (>2 g/dL), confirmed by repeat testing, was significantly lower in patients on celecoxib compared to the NSAID group, relative risk 0.29, 95 % CI 0.17- 0.48. The significantly lower incidence of this event with celecoxib was maintained with or without acetylsalicylic acid use.
In a prospective randomised 24 week safety study in patients who were aged ≥60 years or had a history of gastroduodenal ulcers (users of ASA excluded), the percentages of patients with decreases in haemoglobin (≥2 g/dL) and/or haematocrit (≥10 %) of defined or presumed GI origin were lower in patients treated with celecoxib 200 mg twice daily (N=2238) compared to patients treated with diclofenac SR 75 mg twice daily plus omeprazole 20 mg once daily (N=2246) (0.2 % vs. 1.1 % for defined GI origin, p = 0.004; 0.4 % vs. 2.4 % for presumed GI origin, p = 0.0001). The rates of clinically manifest GI complications such as perforation, obstruction or haemorrhage were very low with no differences between the treatment groups (4-5 per group).
Cardiovascular safety - long-term studies involving subjects with sporadic adenomatous polyps: Two studies involving subjects with sporadic adenomatous polyps were conducted with celecoxib i.e., the APC trial (Adenoma Prevention with Celecoxib) and the PreSAP trial (Prevention of Spontaneous Adenomatous Polyps). In the APC trial, there was a dose-related increase in the composite endpoint of CV death, myocardial infarction, or stroke (adjudicated) with celecoxib compared to placebo over 3 years of treatment. The PreSAP trial did not demonstrate a statistically significant increased risk for the same composite endpoint.
In the APC trial, the relative risks compared to placebo for a composite endpoint (adjudicated) of CV death, myocardial infarction, or stroke were 3.4 (95 % CI 1.4 - 8.5) with celecoxib 400 mg twice daily and 2.8 (95 % CI 1.1 - 7.2) with celecoxib 200 mg twice daily. Cumulative rates for this composite endpoint over 3 years were 3.0 % (20/671 subjects) and 2.5 % (17/685 subjects), respectively, compared to 0.9 % (6/679 subjects) for placebo. The increases for both celecoxib dose groups versus placebo were mainly due to an increased incidence of myocardial infarction.
In the PreSAP trial, the relative risk compared to placebo for this same composite endpoint (adjudicated) was 1.2 (95 % CI 0.6 - 2.4) with celecoxib 400 mg once daily compared to placebo. Cumulative rates for this composite endpoint over 3 years were 2.3 % (21/933 subjects) and 1.9 % (12/628 subjects), respectively. The incidence of myocardial infarction (adjudicated) was 1.0 % (9/933 subjects) with celecoxib 400 mg once daily and 0.6 % (4/628 subjects) with placebo.
Data from a third long-term study, ADAPT (The Alzheimer's Disease Anti-inflammatory Prevention Trial), did not show a significantly increased CV risk with celecoxib 200 mg BID compared to placebo. The relative risk compared to placebo for a similar composite endpoint (CV death, myocardial infarction, stroke) was 1.14 (95 % CI 0.61 - 2.15) with celecoxib 200 mg twice daily. The incidence of myocardial infarction was 1.1 % (8/717 patients) with celecoxib 200 mg twice daily and 1.2 % (13/1070 patients) with placebo.
Pharmacokinetics: Absorption: Celecoxib is well absorbed reaching peak plasma concentrations after approximately 2-3 hours. Dosing with food (high fat meal) delays absorption of celecoxib by about 1 hour resulting in a Tmax of about 4 hours and increases bioavailability by about 20%.
Distribution: Plasma protein binding is about 97 % at therapeutic plasma concentrations and the medicinal product is not preferentially bound to erythrocytes.
Biotransformation: Celecoxib metabolism is primarily mediated via cytochrome P450 2C9. Three metabolites, inactive as COX-1 or COX-2 inhibitors, have been identified in human plasma i.e., a primary alcohol, the corresponding carboxylic acid and its glucuronide conjugate.
Cytochrome P450 2C9 activity is reduced in individuals with genetic polymorphisms that lead to reduced enzyme activity, such as those homozygous for the CYP2C9*3 polymorphism.
In a pharmacokinetic study of celecoxib 200 mg administered once daily in healthy volunteers, genotyped as either CYP2C9*1/*1, CYP2C9*1/*3, or CYP2C9*3/*3, the median Cmax and AUC0-24 of celecoxib on day 7 were approximately 4-fold and 7-fold, respectively, in subjects genotyped as CYP2C9*3/*3 compared to other genotypes. In three separate single dose studies, involving a total of 5 subjects genotyped as CYP2C9*3/*3, single-dose AUC0-24 increased by approximately 3-fold compared to normal metabolisers. It is estimated that the frequency of the homozygous *3/*3 genotype is 0.3-1.0 % among different ethnic groups.
Patients who are known, or suspected to be CYP2C9 poor metabolisers based on previous history/experience with other CYP2C9 substrates should be administered celecoxib with caution (see Dosage & Administration).
No clinically significant differences were found in PK parameters of celecoxib between elderly African-Americans and Caucasians.
The plasma concentration of celecoxib is approximately 100 % increased in elderly women (>65 years).
Compared to subjects with normal hepatic function, patients with mild hepatic impairment had a mean increase in Cmax of 53 % and in AUC of 26 % of celecoxib. The corresponding values in patients with moderate hepatic impairment were 41 % and 146 % respectively. The metabolic capacity in patients with mild to moderate impairment was best correlated to their albumin values. Treatment should be initiated at half the recommended dose in patients with moderate liver impairment (with serum albumin 25-35 g/l). Patients with severe hepatic impairment (serum albumin <25 g/l) have not been studied and celecoxib is contraindicated in this patient group.
There is little experience of celecoxib in renal impairment. The pharmacokinetics of celecoxib has not been studied in patients with renal impairment but is unlikely to be markedly changed in these patients. Thus caution is advised when treating patients with renal impairment. Severe renal impairment is contraindicated.
Elimination: Celecoxib is mainly eliminated by metabolism. Less than 1 % of the dose is excreted unchanged in urine. The inter-subject variability in the exposure of celecoxib is about 10-fold. Celecoxib exhibits dose- and time-independent pharmacokinetics in the therapeutic dose range. Elimination half-life is 8-12 hours. Steady state plasma concentrations are reached within 5 days of treatment.
Toxicology: Preclinical safety data: Conventional embryo-foetal toxicity studies resulted in dose dependent occurrences of diaphragmatic hernia in rat foetuses and of cardiovascular malformations in rabbit foetuses at systemic exposures to free drug approximately 5X (rat) and 3X (rabbit) higher than those achieved at the maximum recommended daily human dose (400 mg). Diaphragmatic hernia was also seen in a peri-post natal toxicity study in rats, which included exposure during the organogenetic period. In the latter study, at the lowest systemic exposure where this anomaly occurred in a single animal, the estimated margin relative to the maximum recommended daily human dose was 3X.
In animals, exposure to celecoxib during early embryonic development resulted in pre-implantation and post-implantation losses. These effects are expected following inhibition of prostaglandin synthesis.
Celecoxib was excreted in rat milk. In a peri-post natal study in rats, pup toxicity was observed.
Based on conventional studies of genotoxicity and carcinogenicity, no special hazard for humans was observed, beyond those addressed in other sections of the monograph. In a two-year toxicity study an increase in nonadrenal thrombosis was observed in male rat at high doses.
Celecoxib Farmoz is indicated in adults for the symptomatic relief in the treatment of osteoarthritis, rheumatoid arthritis and ankylosing spondylitis.
The decision to prescribe a selective cyclooxygenase-2 (COX-2) inhibitor should be based on an assessment of the individual patient's overall risks (see Contraindications and Precautions).
Posology: As the cardiovascular (CV) risks of celecoxib may increase with dose and duration of exposure, the shortest duration possible and the lowest effective daily dose should be used. The patient's need for symptomatic relief and response to therapy should be re-evaluated periodically, especially in patients with osteoarthritis (see Contraindications, Precautions, Adverse Reactions and Pharmacology: Pharmacodynamics under Actions).
Osteoarthritis: The usual recommended daily dose is 200 mg taken once daily or in two divided doses. In some patients, with insufficient relief from symptoms, an increased dose of 200 mg twice daily may increase efficacy. In the absence of an increase in therapeutic benefit after two weeks, other therapeutic options should be considered.
Rheumatoid arthritis: The initial recommended daily dose is 200 mg taken in two divided doses. The dose may, if needed, later be increased to 200 mg twice daily. In the absence of an increase in therapeutic benefit after two weeks, other therapeutic options should be considered.
Ankylosing spondylitis: The recommended daily dose is 200 mg taken once daily or in two divided doses. In a few patients, with insufficient relief from symptoms, an increased dose of 400 mg once daily or in two divided doses may increase efficacy. In the absence of an increase in therapeutic benefit after two weeks, other therapeutic options should be considered.
The maximum recommended daily dose is 400 mg for all indications.
Special populations: Elderly: As in younger adults, 200 mg per day should be used initially. The dose may, if needed, later be increased to 200 mg twice daily. Particular caution should be exercised in elderly with a body weight less than 50 kg (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Paediatric population: Celecoxib is not indicated for use in children.
CYP2C9 poor metabolisers: Patients who are known, or suspected to be CYP2C9 poor metabolisers based on genotyping or previous history/experience with other CYP2C9 substrates should be administered celecoxib with caution as the risk of dose-dependent adverse effects is increased. Consider reducing the dose to half the lowest recommended dose (see Pharmacology: Pharmacokinetics under Actions).
Hepatic impairment: Treatment should be initiated at half the recommended dose in patients with established moderate liver impairment with a serum albumin of 25-35 g/l. Experience in such patients is limited to cirrhotic patients (see Contraindications, Precautions and Pharmacology: Pharmacokinetics under Actions).
Renal impairment: Experience with celecoxib in patients with mild or moderate renal impairment is limited, therefore such patients should be treated with caution (see Contraindications, Precautions and Pharmacology: Pharmacokinetics under Actions).
Method of administration: Oral use: Celecoxib Farmoz may be taken with or without food.
There is no clinical experience of overdose. Single doses up to 1200 mg and multiple doses up to 1200 mg twice daily have been administered to healthy subjects for nine days without clinically significant adverse effects. In the event of suspected overdose, appropriate supportive medical care should be provided e.g. by eliminating the gastric contents, clinical supervision and, if necessary, the institution of symptomatic treatment. Dialysis is unlikely to be an efficient method of medicinal product removal due to high protein binding.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Known hypersensitivity to sulfonamides.
Active peptic ulceration or gastrointestinal (GI) bleeding.
Patients who have experienced asthma, acute rhinitis, nasal polyps, angioneurotic oedema, urticaria or other allergic-type reactions after taking acetylsalicylic acid (aspirin) or other non-steroidal anti-inflammatory drugs (NSAIDs) including COX-2 inhibitors.
In pregnancy and in women of childbearing potential unless using an effective method of contraception (see Use in Pregnancy & Lactation). Celecoxib has been shown to cause malformations in the two animal species studied (see Use in Pregnancy & Lactation and Pharmacology: Toxicology: Preclinical safety data under Actions). The potential for human risk in pregnancy is unknown, but cannot be excluded.
Breast-feeding (see Use in Pregnancy & Lactation and Pharmacology: Toxicology: Preclinical safety data under Actions).
Severe hepatic dysfunction (serum albumin <25 g/l or Child-Pugh score ≥10).
Patients with estimated creatinine clearance <30 ml/min.
Inflammatory bowel disease.
Congestive heart failure (NYHA II-IV).
Established ischaemic heart disease, peripheral arterial disease and/or cerebrovascular disease.
Gastrointestinal (GI) effects: Upper and lower gastrointestinal complications (perforations, ulcers or bleedings [PUBs]), some of them resulting in fatal outcome, have occurred in patients treated with celecoxib. Caution is advised with treatment of patients most at risk of developing a gastrointestinal complication with NSAIDs; the elderly, patients using any other NSAID or antiplatelet drugs (such as acetylsalicylic acid) or glucocorticoids concomitantly, patients using alcohol, or patients with a prior history of gastrointestinal disease, such as ulceration and GI bleeding.
There is further increase in the risk of gastrointestinal adverse effects for celecoxib (gastrointestinal ulceration or other gastrointestinal complications), when celecoxib is taken concomitantly with acetylsalicylic acid (even at low doses).
A significant difference in GI safety between selective COX-2 inhibitors + acetylsalicylic acid vs. NSAIDs + acetylsalicylic acid has not been demonstrated in long-term clinical trials (see Pharmacology: Pharmacodynamics under Actions).
Concomitant NSAID use: The concomitant use of celecoxib and a non-aspirin NSAID should be avoided.
Cardiovascular effects: Increased number of serious cardiovascular (CV) events, mainly myocardial infarction, has been found in a long-term placebo-controlled study in subjects with sporadic adenomatous polyps treated with celecoxib at doses of 200 mg BID and 400 mg BID compared to placebo (see Pharmacology: Pharmacodynamics under Actions).
As the cardiovascular risks of celecoxib may increase with dose and duration of exposure, the shortest duration possible and the lowest effective daily dose should be used. NSAIDs, including COX-2 selective inhibitors, have been associated with increased risk of cardiovascular and thrombotic adverse events when taken long term. The exact magnitude of the risk associated with a single dose has not been determined, nor has the exact duration of therapy associated with increased risk. The patient's need for symptomatic relief and response to therapy should be re-evaluated periodically, especially in patients with osteoarthritis (see Dosage & Administration, Contraindications, Adverse Reactions and Pharmacology: Pharmacodynamics under Actions).
Patients with significant risk factors for cardiovascular events (e.g. hypertension, hyperlipidaemia, diabetes mellitus, smoking) should only be treated with celecoxib after careful consideration (see Pharmacology: Pharmacodynamics under Actions).
COX-2 selective inhibitors are not a substitute for acetylsalicylic acid for prophylaxis of cardiovascular thrombo-embolic diseases because of their lack of antiplatelet effects. Therefore, antiplatelet therapies should not be discontinued (see Pharmacology: Pharmacodynamics under Actions).
Fluid retention and oedema: As with other medicinal products known to inhibit prostaglandin synthesis, fluid retention and oedema have been observed in patients taking celecoxib. Therefore, celecoxib should be used with caution in patients with history of cardiac failure, left ventricular dysfunction or hypertension, and in patients with pre-existing oedema from any other reason, since prostaglandin inhibition may result in deterioration of renal function and fluid retention. Caution is also required in patients taking diuretic treatment or otherwise at risk of hypovolaemia.
Hypertension: As with all NSAIDS, celecoxib can lead to the onset of new hypertension or worsening of pre-existing hypertension, either of which may contribute to the increased incidence of cardiovascular events. Therefore, blood pressure should be monitored closely during the initiation of therapy with celecoxib and throughout the course of therapy.
Hepatic and renal effects: Compromised renal or hepatic function and especially cardiac dysfunction are more likely in the elderly and therefore medically appropriate supervision should be maintained.
NSAIDs, including celecoxib, may cause renal toxicity. Clinical trials with celecoxib have shown renal effects similar to those observed with comparator NSAIDs. Patients at greatest risk for renal toxicity are those with impaired renal function, heart failure, liver dysfunction, those taking diuretics, angiotensin converting enzyme (ACE)-inhibitors, angiotensin II receptor antagonists, and the elderly (see Interactions). Such patients should be carefully monitored while receiving treatment with celecoxib.
Some cases of severe hepatic reactions, including fulminant hepatitis (some with fatal outcome), liver necrosis and, hepatic failure (some with fatal outcome or requiring liver transplant), have been reported with celecoxib. Among the cases that reported time to onset, most of the severe adverse hepatic events developed within one month after initiation of celecoxib treatment (see Adverse Reactions).
If during treatment, patients deteriorate in any of the organ system functions described previously, appropriate measures should be taken and discontinuation of celecoxib therapy should be considered.
CYP2D6 inhibition: Celecoxib inhibits CYP2D6. Although it is not a strong inhibitor of this enzyme, a dose reduction may be necessary for individually dose-titrated medicinal products that are metabolised by CYP2D6 (see Interactions).
CYP2C9 poor metabolisers: Patients known to be CYP2C9 poor metabolisers should be treated with caution (see Pharmacology: Pharmacokinetics under Actions).
Skin and systemic hypersensitivity reactions: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome, and toxic epidermal necrolysis, have been reported very rarely in association with the use of celecoxib (see Adverse Reactions). Patients appear to be at highest risk for these reactions early in the course of therapy: the onset of the reaction occurring in the majority of cases within the first month of treatment. Serious hypersensitivity reactions (including anaphylaxis, angioedema and drug rash with eosinophilia and systemic symptoms (DRESS), or hypersensitivity syndrome), have been reported in patients receiving celecoxib (see Adverse Reactions). Patients with a history of sulfonamide allergy or any drug allergy may be at greater risk of serious skin reactions or hypersensitivity reactions (see Contraindications). Celecoxib should be discontinued at the first appearance of skin rash, mucosal lesions, or any other sign of hypersensitivity.
General: Celecoxib may mask fever and other signs of inflammation.
Use with oral anticoagulants: In patients on concurrent therapy with warfarin, serious bleeding events, some of them fatal, have been reported. Increased prothrombin time (INR) with concurrent therapy has been reported. Therefore, this should be closely monitored in patients receiving warfarin/coumarin-type oral anticoagulants, particularly when therapy with celecoxib is initiated or celecoxib dose is changed (see Interactions). Concomitant use of anticoagulants with NSAIDS may increase the risk of bleeding. Caution should be exercised when combining celecoxib with warfarin or other oral anticoagulants, including novel anticoagulants (e.g. apixaban, dabigatran, and rivaroxaban).
Excipients: Celecoxib Farmoz 100 mg and 200 mg capsules contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Patients who experience dizziness, vertigo or somnolence while taking Celecoxib Farmoz should refrain from driving or operating machinery.
Pregnancy: Studies in animals (rats and rabbits) have shown reproductive toxicity, including malformations (see Contraindications and Pharmacology: Toxicology: Preclinical safety data under Actions). Inhibition of prostaglandin synthesis might adversely affect pregnancy. Data from epidemiological studies suggest an increased risk of spontaneous abortion after use of prostaglandin synthesis inhibitors in early pregnancy. The potential for human risk in pregnancy is unknown, but cannot be excluded. Celecoxib, as with other medicinal products inhibiting prostaglandin synthesis, may cause uterine inertia and premature closure of the ductus arteriosus during the last trimester.
During the second or third trimester of pregnancy, NSAIDs including celecoxib may cause fetal renal dysfunction which may result in reduction of amniotic fluid volume or oligohydramnios in severe cases. Such effects may occur shortly after treatment initiation and are usually reversible.
Celecoxib is contraindicated in pregnancy and in women who can become pregnant (see Contraindications and Precautions). If a woman becomes pregnant during treatment, celecoxib should be discontinued.
Breast-feeding: Celecoxib is excreted in the milk of lactating rats at concentrations similar to those in plasma. Administration of celecoxib to a limited number of lactating women has shown a very low transfer of celecoxib into breast milk. Women who take Celecoxib Farmoz should not breastfeed.
Fertility: Based on the mechanism of action, the use of NSAIDs, including celecoxib, may delay or prevent rupture of ovarian follicles, which has been associated with reversible infertility in some women.
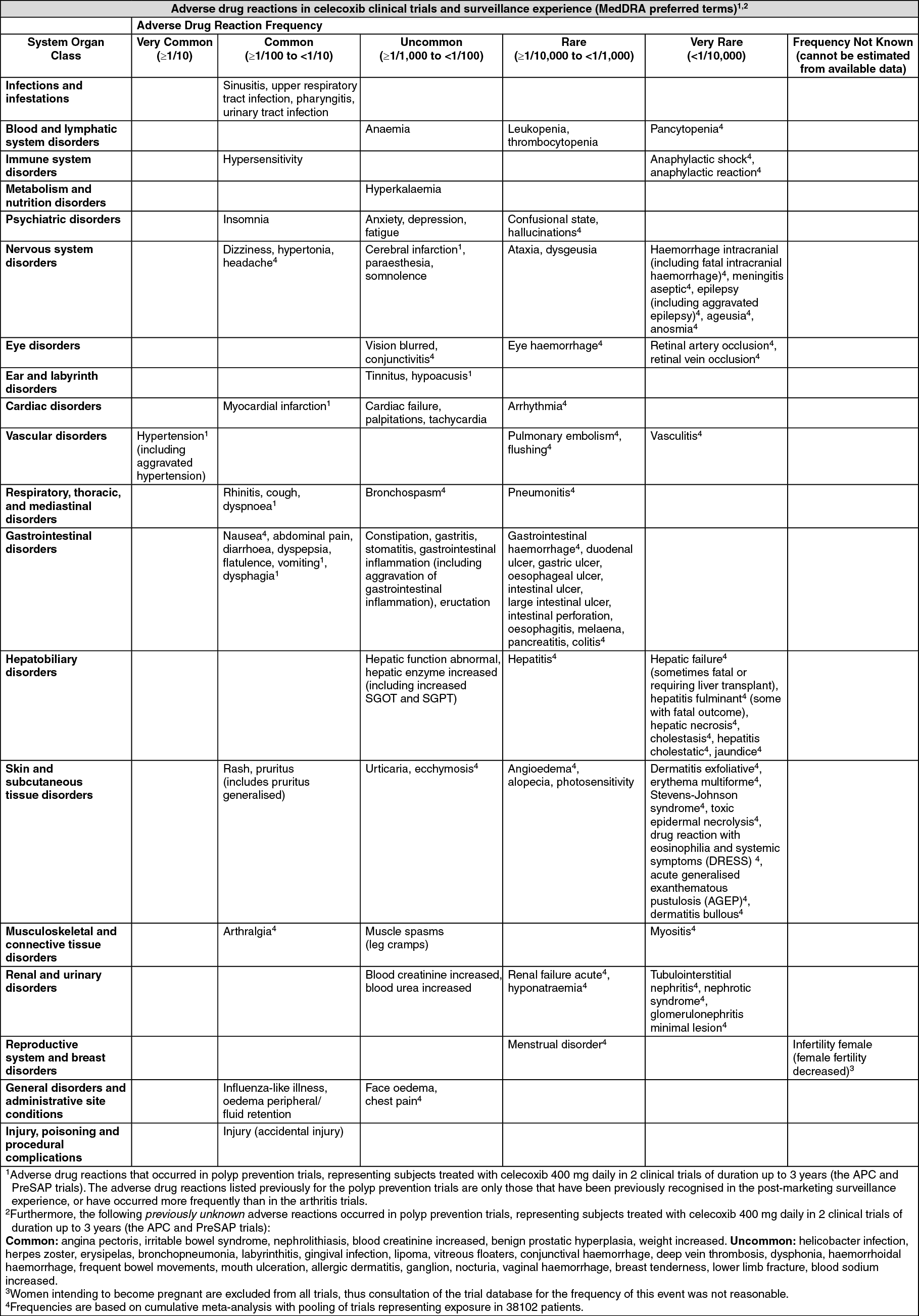
Adverse reactions are listed by system organ class and ranked by frequency in the table, reflecting data from the following sources: Adverse reactions reported in osteoarthritis patients and rheumatoid arthritis patients at incidence rates greater than 0.01 % and greater than those reported for placebo during 12 placebo- and/or active-controlled clinical trials of duration up to 12 weeks at celecoxib daily doses from 100 mg up to 800 mg. In additional studies using non-selective NSAID comparators, approximately 7400 arthritis patients have been treated with celecoxib at daily doses up to 800 mg, including approximately 2300 patients treated for 1 year or longer. The adverse reactions observed with celecoxib in these additional studies were consistent with those for osteoarthritis and rheumatoid arthritis patients listed in the table.
Adverse reactions reported at incidence rates greater than placebo for subjects treated with celecoxib 400 mg daily in long-term polyp prevention trials of duration up to 3 years (the Adenoma Prevention with Celecoxib (APC) and Prevention of Colorectal Sporadic Adenomatous Polyps (PreSAP) trials; see Pharmacology: Pharmacodynamics: Cardiovascular safety - long-term studies involving patients with sporadic adenomatous polyps under Actions).
Adverse drug reactions from post-marketing surveillance as spontaneously reported during a period in which an estimated >70 million patients were treated with celecoxib (various doses, durations, and indications). Even though these were identified as reactions from post-marketing reports, trial data was consulted to estimate frequency. Frequencies are based on a cumulative meta-analysis with pooling of trials representing exposure in 38102 patients. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In final data (adjudicated) from the APC and PreSAP trials in patients treated with celecoxib 400 mg daily for up to 3 years (pooled data from both trials; see Pharmacology: Pharmacodynamics under Actions for results from individual trials), the excess rate over placebo for myocardial infarction was 7.6 events per 1,000 patients (uncommon) and there was no excess rate for stroke (types not differentiated) over placebo.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
Pharmacodynamic interactions: Anticoagulants: Anticoagulant activity should be monitored particularly in the first few days after initiating or changing the dose of celecoxib in patients receiving warfarin or other anticoagulants since these patients have an increased risk of bleeding complications. Therefore, patients receiving oral anticoagulants should be closely monitored for their prothrombin time INR, particularly in the first few days when therapy with celecoxib is initiated or the dose of celecoxib is changed (see Precautions). Bleeding events in association with increases in prothrombin time have been reported, predominantly in the elderly, in patients receiving celecoxib concurrently with warfarin, some of them fatal.
Anti-hypertensives: NSAIDs may reduce the effect of anti-hypertensive medicinal products including ACE-inhibitors, angiotensin II receptor antagonists, diuretics and beta-blockers. As for NSAIDs, the risk of acute renal insufficiency, which is usually reversible, may be increased in some patients with compromised renal function (e.g. dehydrated patients, patients on diuretics, or elderly patients) when ACE-inhibitors, angiotensin II receptor antagonists, and/or diuretics are combined with NSAIDs, including celecoxib (see Precautions). Therefore, the combination should be administered with caution, especially in the elderly. Patients should be adequately hydrated and consideration should be given to monitoring of renal function after initiation of concomitant therapy, and periodically thereafter.
In a 28-day clinical study in patients with lisinopril-controlled Stage I and II hypertension, administration of celecoxib 200 mg BID resulted in no clinically significant increases, when compared to placebo treatment, in mean daily systolic or diastolic blood pressure as determined using 24-hour ambulatory blood pressure monitoring. Among patients treated with celecoxib 200 mg BID, 48 % were considered unresponsive to lisinopril at the final clinic visit (defined as either cuff diastolic blood pressure >90 mmHg or cuff diastolic blood pressure increased >10 % compared to baseline), compared to 27 % of patients treated with placebo; this difference was statistically significant.
Ciclosporin and tacrolimus: Co-administration of NSAIDs and ciclosporin or tacrolimus may increase the nephrotoxic effect of ciclosporin or tacrolimus, respectively. Renal function should be monitored when celecoxib and any of these medicinal products are combined.
Acetylsalicylic acid: Celecoxib can be used with low-dose acetylsalicylic acid but is not a substitute for acetylsalicylic acid for CV prophylaxis. In the submitted studies, as with other NSAIDs, an increased risk of gastrointestinal ulceration or other gastrointestinal complications compared to use of celecoxib alone was shown for concomitant administration of low-dose acetylsalicylic acid (see Pharmacology: Pharmacodynamics under Actions).
Pharmacokinetic interactions: Effects of celecoxib on other medicinal products: CYP2D6 inhibition: Celecoxib is an inhibitor of CYP2D6. The plasma concentrations of medicinal products that are substrates of this enzyme may be increased when celecoxib is used concomitantly. Examples of medicinal products which are metabolised by CYP2D6 are antidepressants (tricyclics and SSRIs), neuroleptics, anti-arrhythmic medicinal products, etc. The dose of individually dose-titrated CYP2D6 substrates may need to be reduced when treatment with celecoxib is initiated or increased if treatment with celecoxib is terminated.
Concomitant administration of celecoxib 200 mg twice daily resulted in 2.6-fold and 1.5-fold increases in plasma concentrations of dextromethorphan and metoprolol (CYP2D6 substrates), respectively. These increases are due to celecoxib inhibition of the CYP2D6 substrate metabolism.
CYP2C19 inhibition: In vitro studies have shown some potential for celecoxib to inhibit CYP2C19 catalysed metabolism. The clinical significance of this in vitro finding is unknown. Examples of medicinal products which are metabolised by CYP2C19 are diazepam, citalopram and imipramine.
Methotrexate: In patients with rheumatoid arthritis celecoxib had no statistically significant effect on the pharmacokinetics (plasma or renal clearance) of methotrexate (in rheumatologic doses). However, adequate monitoring for methotrexate-related toxicity should be considered when combining these two medicinal products.
Lithium: In healthy subjects, co-administration of celecoxib 200 mg twice daily with 450 mg twice daily of lithium resulted in a mean increase in Cmax of 16 % and in area under the curve (AUC) of 18 % of lithium. Therefore, patients on lithium treatment should be closely monitored when celecoxib is introduced or withdrawn.
Oral contraceptives: In an interaction study, celecoxib had no clinically relevant effects on the pharmacokinetics of oral contraceptives (1 mg norethisterone /35 micrograms ethinylestradiol).
Glibenclamide/tolbutamide: Celecoxib does not affect the pharmacokinetics of tolbutamide (CYP2C9 substrate), or glibenclamide to a clinically relevant extent.
Effects of other medicinal products on celecoxib: CYP2C9 poor metabolisers: In individuals who are CYP2C9 poor metabolisers and demonstrate increased systemic exposure to celecoxib, concomitant treatment with CYP2C9 inhibitors such as fluconazole could result in further increases in celecoxib exposure. Such combinations should be avoided in known CYP2C9 poor metabolisers (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions).
CYP2C9 inhibitors and inducers: Since celecoxib is predominantly metabolised by CYP2C9 it should be used at half the recommended dose in patients receiving fluconazole. Concomitant use of 200 mg single dose of celecoxib and 200 mg once daily of fluconazole, a potent CYP2C9 inhibitor, resulted in a mean increase in celecoxib Cmax of 60% and in AUC of 130%. Concomitant use of inducers of CYP2C9 such as rifampicin, carbamazepine and barbiturates may reduce plasma concentrations of celecoxib.
Ketoconazole and antacids: Ketoconazole or antacids have not been observed to affect the pharmacokinetics of celecoxib.
Paediatric population: Interaction studies have only been performed in adults.
Special precautions for disposal and other handling: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Not applicable.
M01AH01 - celecoxib ; Belongs to the class of non-steroidal antiinflammatory and antirheumatic products, coxibs.
Celecoxib Farmoz cap 200 mg
1 × 20's;3 × 20's
Celecoxib Farmoz cap 100 mg
1 × 20's;3 × 20's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out